Gastric Sleeve vs Mini Gastric Bypass 2026: Which Is Right For You?
Gastric Sleeve vs Mini Gastric Bypass 2026: A Surgeon's Perspective
The two most common bariatric operations performed in 2026 are laparoscopic sleeve gastrectomy (gastric sleeve) and one-anastomosis (mini) gastric bypass. Together they account for over 80% of all weight-loss surgeries worldwide. They both work — but they work in different ways, and the right choice depends on your BMI, your reflux history, whether you have type 2 diabetes, and how much complexity you are willing to accept in exchange for better long-term results.
This guide breaks down the real differences in 2026 — using current evidence and the day-to-day experience of operating on thousands of international patients in Istanbul.
In This Article
- How sleeve and mini bypass actually work in 2026
- Side-by-side weight loss, diabetes and reflux data
- Cost, recovery and reversibility compared
- Who should pick sleeve, who should pick mini bypass
- A decision matrix you can use today
How the Gastric Sleeve Works
In a sleeve gastrectomy, the surgeon removes about 75–80% of the stomach along the greater curvature, leaving behind a long, narrow tube — the "sleeve". The pylorus and intestines stay completely untouched. The operation is purely restrictive (smaller stomach) and hormonal (the removed fundus produces 80–90% of the body's ghrelin, the hunger hormone).
It is the most popular operation in the world for a reason: it is technically simpler, has no rerouting of intestines, takes 45–60 minutes, and produces excellent weight loss with minimal long-term nutritional issues.
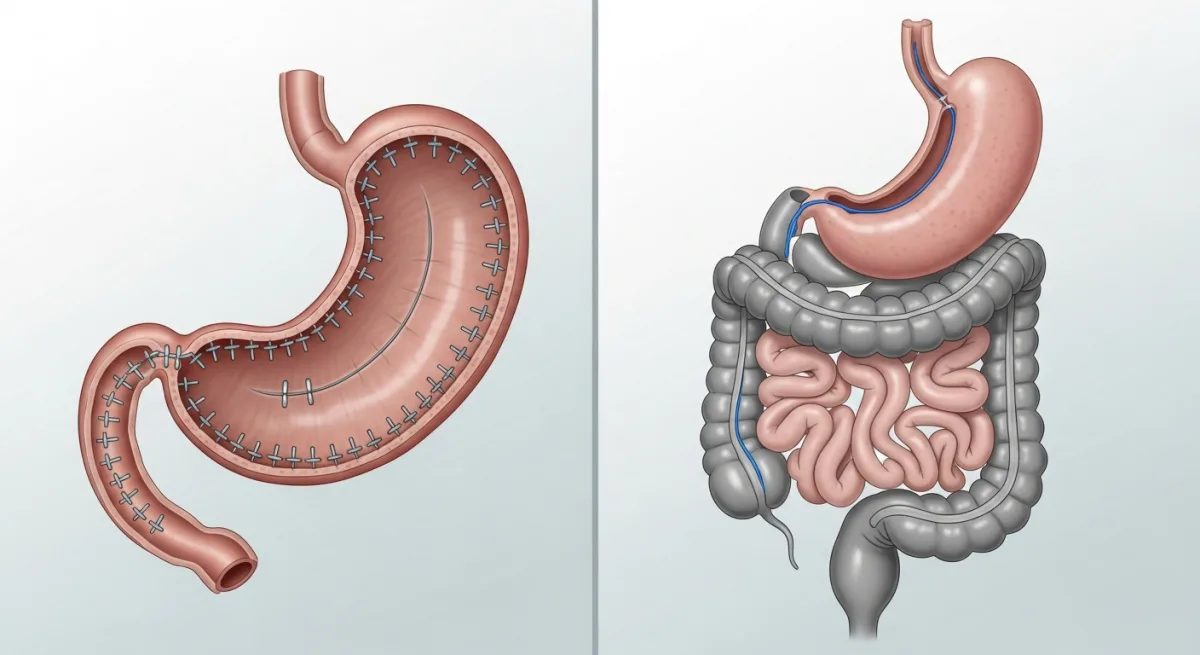
How the Mini Gastric Bypass Works
The mini gastric bypass (also called one-anastomosis gastric bypass, or OAGB) creates a long, narrow stomach pouch — similar in shape to a sleeve — and then connects that pouch directly to a loop of small intestine roughly 150–200 cm beyond the natural connection. Food bypasses the duodenum and the upper part of the jejunum.
This produces three effects: restriction (smaller pouch), malabsorption (less surface area for calorie absorption), and strong metabolic/hormonal change (the rerouting itself triggers gut hormones that improve insulin sensitivity dramatically). The operation takes 75–90 minutes.
To compare with the classic Roux-en-Y bypass, see our complete treatments page.
Head-to-Head: The 2026 Numbers
| Metric | Gastric Sleeve | Mini Gastric Bypass |
|---|---|---|
| % Total Body Weight Loss at 12 months | 28–32% | 32–38% |
| % TBWL at 5 years | 22–26% | 26–30% |
| Type 2 diabetes remission | 55–65% | 75–85% |
| Reflux improvement | Can worsen | Usually improves |
| Operation time | 45–60 min | 75–90 min |
| Hospital stay | 2 nights | 2 nights |
| Vitamin supplementation | Multivitamin lifelong | Multi + B12 + iron + calcium |
| Reversibility | Permanent | Reversible |
| Cost from (Istanbul) | £2,950 | £3,350 |
If You Have Type 2 Diabetes
The single biggest difference is metabolic impact. Mini gastric bypass causes a significant rerouting of food past the duodenum, which triggers powerful gut-hormone changes (GLP-1, PYY, GIP) and improves insulin sensitivity within days — long before any meaningful weight loss. Diabetes remission rates of 75–85% at one year are the published norm, with many patients off all glucose-lowering medication within 2–4 weeks.
Sleeve gastrectomy also improves diabetes (55–65% remission), but the effect is slower and more weight-loss-dependent. If you have type 2 diabetes — especially if you are insulin-dependent — mini bypass is usually the better choice.
If You Have Reflux (GERD)
Sleeve gastrectomy can worsen reflux. The smaller, higher-pressure tube of the sleeve sometimes pushes acid up against the lower oesophagus, and 15–20% of sleeve patients develop new or worse reflux. Mini bypass, by contrast, removes acid-producing tissue from the food pathway and typically improves reflux. If you already take daily PPIs, mini bypass is safer.
If Your BMI Is Very High
Patients with BMI 50+ tend to do better long-term with bypass operations. The combination of restriction, malabsorption and metabolic effect produces deeper weight loss with lower regain rates. For patients with BMI 40–50, both operations work well; for BMI 35–40, sleeve is often the more proportionate choice.
If You Want the Simplest Operation
Sleeve is faster, technically simpler, has no anastomosis (intestinal join), no internal hernia risk, no marginal ulcer risk and the lowest lifelong supplementation burden. For BMI 35–45 with no reflux and no diabetes, sleeve is usually the right answer.
Side Effects and Risks
Sleeve
- New-onset reflux in 15–20%
- Leak risk under 1% in experienced centres
- Hair shedding at month 3–6 (temporary)
- Low long-term nutritional deficiency risk
Mini Gastric Bypass
- Bile reflux in 1–3% (managed surgically if needed)
- Marginal ulcer risk if NSAIDs or smoking continue
- Slightly higher risk of B12, iron and calcium deficiency — managed with lifelong supplementation
- Dumping syndrome possible after sugary foods (usually a positive aversive learning loop)
Long-Term Reversibility
This is one of the most underappreciated factors. Sleeve gastrectomy permanently removes 75–80% of the stomach. There is no going back. Mini bypass does not remove any organ — the bypass can be reversed if there is a serious problem, restoring near-normal anatomy. For some patients, especially younger ones, this matters.
Decision Matrix
| Your Situation | Better Choice |
|---|---|
| BMI 35–40, no diabetes, no reflux | Sleeve |
| BMI 40–50 with type 2 diabetes | Mini bypass |
| BMI 50+ regardless of comorbidities | Mini bypass |
| Severe reflux / hiatus hernia | Mini bypass |
| Younger patient wanting reversibility | Mini bypass |
| Want lowest vitamin burden | Sleeve |
Frequently Asked Questions
Can I switch from sleeve to mini bypass later?
Yes — sleeve to bypass is one of the most common revisions, usually for severe reflux or weight regain. Read more in our revision surgery guide.
Is mini bypass riskier than classic Roux-en-Y bypass?
Modern data shows comparable safety, with mini bypass actually offering slightly shorter operating time and lower internal hernia risk because there is only one anastomosis instead of two.
Will I dump after every meal with mini bypass?
No — dumping is triggered by concentrated sugar and high-glycaemic carbs. With a balanced protein-led diet, most patients rarely experience symptoms.
Which one will I lose more weight with?
On average, mini bypass produces 4–6% more total body weight loss at every time point. For an individual patient, lifestyle adherence matters more than procedure choice.
Get a Personalised Surgical Recommendation
Send us your BMI, age, comorbidities and reflux history — Dr Murat Ustun's team will reply within 24 hours with a clear procedure recommendation.
Free Eligibility Assessment →Related reading: