Barrett's Esophagus and Increased Risk After Sleeve Gastrectomy
Barrett's Esophagus After Sleeve Gastrectomy: What You Need to Know
Barrett's Esophagus is a serious consequence of long-term acid reflux that can develop in patients who have undergone sleeve gastrectomy. Recent research has shed new light on this important topic, helping patients and healthcare providers better understand the risks and prevention strategies.
What is Barrett's Esophagus?
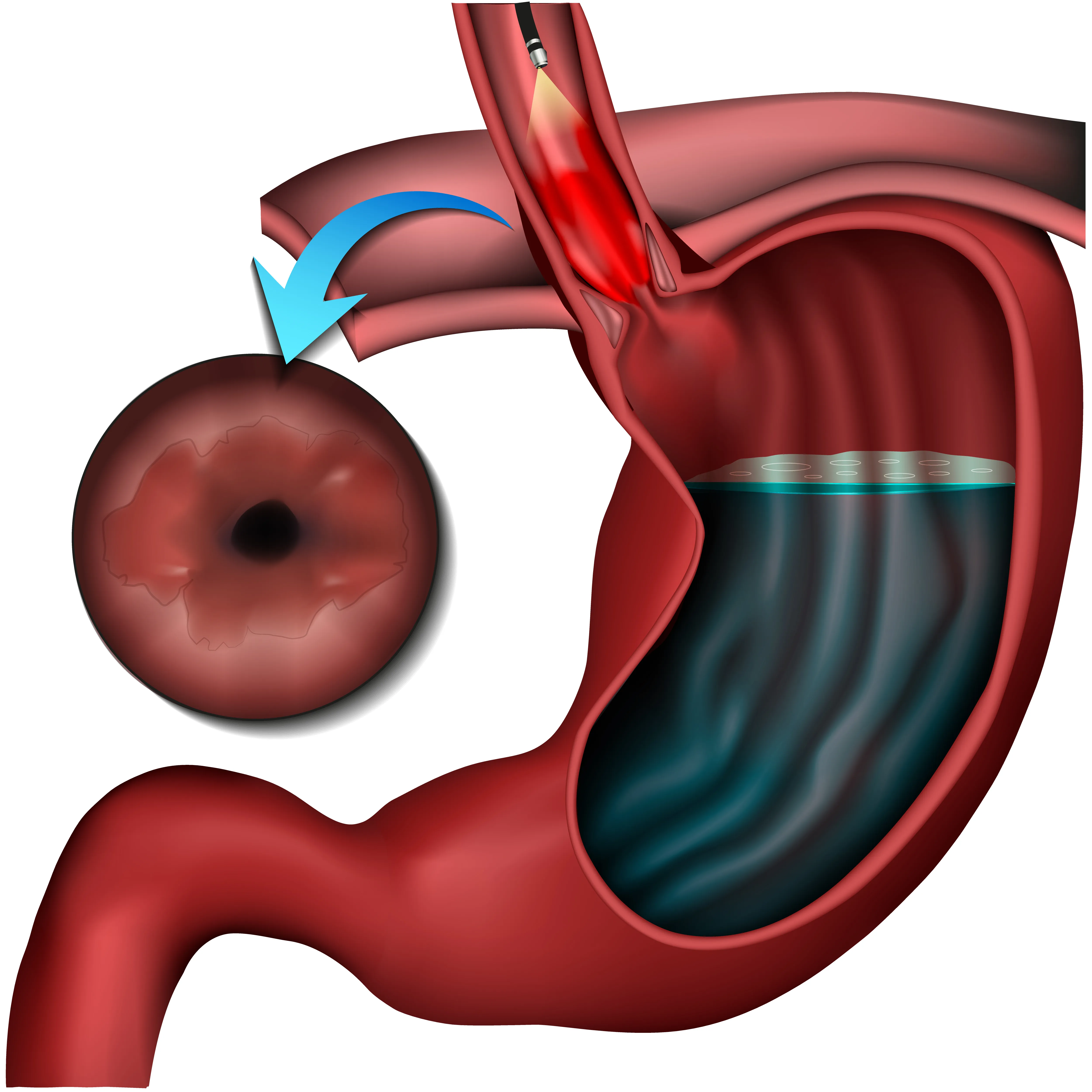
Barrett's Esophagus is a condition where the normal tissue lining the esophagus changes to tissue that resembles the lining of the intestine. This transformation, called intestinal metaplasia, occurs as a response to chronic acid exposure. While Barrett's Esophagus itself doesn't cause symptoms, it is significant because it can be a precursor to esophageal adenocarcinoma, a type of esophageal cancer.
Latest Research Findings (2024 Meta-Analysis)
A comprehensive 2024 meta-analysis published in Clinical Gastroenterology and Hepatology by Chandan et al. analyzed 19 studies involving 2,046 patients with follow-up periods ranging from 2 to 11.4 years. The study revealed several key findings:
- De novo Barrett's Esophagus rate: 5.6% of sleeve gastrectomy patients developed new-onset Barrett's Esophagus
- All cases were non-dysplastic: This means the cellular changes had not progressed to precancerous stages
- Erosive esophagitis: Showed a 13% annual increase post-surgery
- GERD symptoms: Significantly increased despite higher PPI (proton pump inhibitor) use
Time-Dependent Risk Factors
One of the most important findings from recent research is that Barrett's Esophagus risk increases with longer follow-up periods:
- Most Barrett's cases were observed after 3 or more years post-surgery
- Patients beyond 10 years post-surgery showed the highest risk
- The risk appears to be progressive over time, emphasizing the importance of long-term surveillance
Why Sleeve Gastrectomy Increases Risk
The sleeve gastrectomy procedure can increase the risk of acid reflux through several mechanisms:
- Increased gastric pressure: The reduced stomach size leads to higher internal pressure
- Altered anatomy: Changes to the lower esophageal sphincter function
- Hiatal hernia development: Can occur or worsen after surgery
- Reduced gastric compliance: The smaller stomach may push contents upward
Real-World Database Findings
A Colorado statewide database analysis found concerning patterns:
- Only 35% of sleeve gastrectomy patients ever had post-operative endoscopy
- Among those screened at 5 years: 6.4% had Barrett's esophagus and 85% had erosive esophagitis
- These rates were higher than expected given pre-operative rates
Important: Barrett's Can Develop Without Symptoms
Perhaps most significantly, research shows that Barrett's Esophagus can develop even without reflux symptoms. There was no significant correlation between Barrett's development and symptomatic GERD. This means patients may have endoscopic findings without any clinical complaints, making routine surveillance essential.
Who Should Consider Alternative Procedures?
For certain patients, Roux-en-Y gastric bypass may be a better choice than sleeve gastrectomy:
- Patients with pre-existing large hiatal hernia
- Those with pre-existing Barrett's esophagus
- Patients with severe pre-operative GERD
Prevention and Monitoring Recommendations
Based on the latest research, the following recommendations are important for sleeve gastrectomy patients:
- Routine endoscopic surveillance: Recommended for ALL sleeve gastrectomy patients, regardless of symptoms
- Increased screening frequency: Especially for patients more than 10 years post-surgery
- PPI management: Proton pump inhibitors are recommended for GERD and erosive esophagitis control
- Lifestyle modifications: Avoiding late-night eating, maintaining head elevation during sleep, and weight management
- Regular follow-up: Even asymptomatic patients require ongoing monitoring
Comparison: Sleeve Gastrectomy vs. Gastric Bypass
Research comparing the two procedures shows important differences in reflux outcomes:
- Sleeve gastrectomy shows higher rates of post-operative GERD
- Roux-en-Y gastric bypass actually improves reflux symptoms in most patients
- For patients with pre-existing reflux disease, bypass may be the preferred option
Conclusion
While sleeve gastrectomy remains an effective weight loss procedure with many benefits, patients and healthcare providers must be aware of the increased risk of Barrett's Esophagus. The key takeaway from 2024 research is that routine endoscopic surveillance is now recommended for all sleeve gastrectomy patients, particularly those beyond 10 years post-surgery. Early detection and appropriate management can prevent progression to more serious conditions.
If you've had sleeve gastrectomy, discuss your screening schedule with your healthcare provider to ensure you receive appropriate monitoring for Barrett's Esophagus.