GFMA: A New Era in Non‑Surgical Weight Loss
Obesity is a chronic, lifelong disease that often resists diet and exercise alone. Bariatric surgery has been the gold standard for substantial weight loss, but many patients are reluctant to undergo an operation. What if an endoscopic procedure could curb hunger and achieve surgical-level weight loss – all without any incisions? Recent studies (the ABLATE I and ABLATE II trials) suggest this may be possible.
These trials explored a novel technique called gastric fundus mucosal ablation (GFMA), especially in combination with endoscopic sleeve gastroplasty (ESG), and the results are very promising. Patients experienced significant weight loss, dramatic reductions in hunger hormones, and improved appetite control – approaching outcomes seen with surgical sleeve gastrectomy, but via a scar-free outpatient procedure.
What is GFMA and How Does It Work?
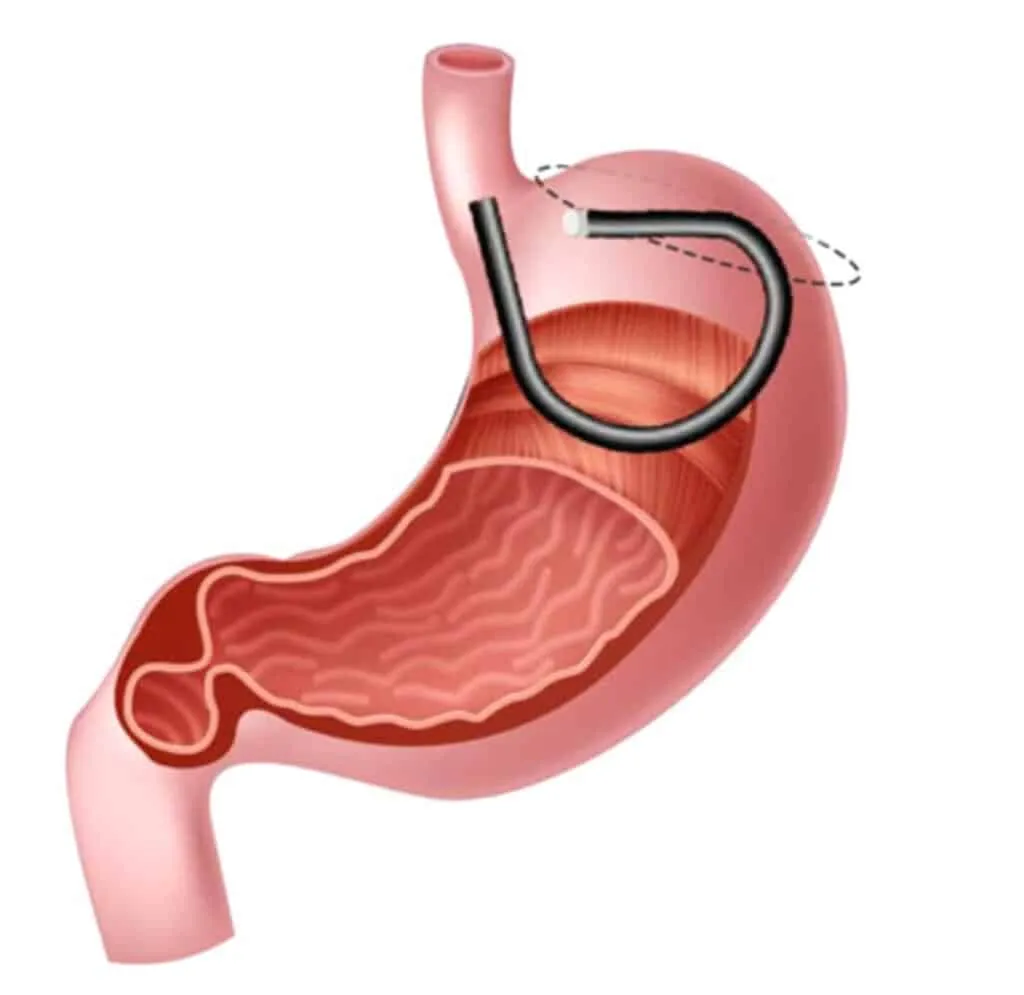
GFMA is an endoscopic procedure that burns the inner lining of the stomach's fundus (the upper pouch of the stomach) in a controlled manner. This might sound intense, but it's done from inside the stomach using a flexible endoscope and specialized tools – no external cuts required. The fundus is a key player in appetite: its mucosa produces about 80–90% of the body's ghrelin, the so-called "hunger hormone," and the fundus also expands to accommodate food and signal fullness. By ablating (destroying) the fundal mucosa, GFMA directly targets hunger at its source.
The mechanism here is similar to what happens in a surgical sleeve gastrectomy (VSG), where the fundus is removed entirely. In both cases, ghrelin levels drop and the stomach's capacity is reduced, leading to decreased appetite and earlier satiety. Importantly, GFMA achieves this without removing any organs – it simply remodels the existing stomach lining.
ABLATE I Trial – First Human Results
The initial human study of GFMA (a pilot trial) was presented in 2024 and involved 10 adults with obesity. The results at 6 months post-procedure were very encouraging:
- Meaningful Weight Loss: Patients lost ~8% of their total body weight on average (about 9 kg or 20 lbs in six months).
- Hunger Hormone Plummeted: Fasting ghrelin levels dropped by ~48% after GFMA – from roughly 460 pg/mL before the procedure to about 250 pg/mL at six months.
- Smaller Stomach Capacity: The functional size of the stomach fundus shrank significantly. A standard liquid fullness test showed 42% less stomach volume could be tolerated post-procedure.
- Less Hunger and "Food Noise": Patients reported a marked decrease in hunger levels and cravings after GFMA.
- Safe and Well-Tolerated: There were zero complications or serious adverse events in the pilot trial.
ABLATE II – Combining GFMA with ESG for Maximum Impact
With the success of the first trial, researchers moved to augment GFMA's effects by pairing it with an endoscopic sleeve gastroplasty. The idea was to perform ESG + GFMA together in one session, creating a powerful one-two punch: the ESG physically restricts intake, while the GFMA curbs hunger hormonally.
The ESG+GFMA combination achieved an average total body weight loss of about 23–24% – essentially surgical-level weight loss without surgery. For context, a typical surgical sleeve gastrectomy often yields roughly 20–25% total body weight loss at one year on average.
How Does GFMA Compare to Surgical Sleeve Gastrectomy?
GFMA with ESG aims to mimic these effects without actual surgery. In lieu of cutting out the fundus, GFMA "inactivates" it by burning the mucosal layer (which holds the ghrelin cells). ESG, meanwhile, mimics the restrictive aspect by suturing the stomach smaller.
Key differences:
- Invasiveness: ESG+GFMA is done through the mouth endoscopically, so no incisions, no stomach stapling, and no removal of organs.
- Hormone Impact: VSG often causes a larger initial drop in ghrelin since the majority of ghrelin-producing cells are literally cut away. GFMA achieves a substantial reduction (~50%).
- Long-Term Durability: Surgical sleeves have long-term data showing maintenance of weight loss for many years. For GFMA, ongoing studies will track patients at 12, 24 months and beyond.
In summary, GFMA (especially paired with ESG) is emerging as a non-surgical alternative to the surgical sleeve. It imitates the sleeve's mechanism – reducing stomach size and hunger – from the inside, with the trade-off of being less invasive but needing further research on long-term effects.